Learn the signs of poor circulation, treatment options and when to seek a second opinion.

Table of Contents


Dr Tay Jia Sheng is a distinguished vascular surgeon in Singapore, specialising in minimally invasive vascular, endovascular and endovenous procedures. He treats a broad range of conditions including varicose veins, deep vein thrombosis, peripheral arterial disease, diabetic foot ulcers and aortic aneurysms.
As a founding vascular surgeon at Sengkang General Hospital, Dr Tay led one of Singapore’s busiest vascular units with strong outcomes and low complication rates. He is among the few local surgeons skilled in advanced techniques such as minimally invasive vein harvesting and complex endovascular aneurysm repairs.
Outside the operating theatre, he has taught at Yong Loo Lin, Duke-NUS and Lee Kong Chian medical schools. Recognised with awards such as the SingHealth Quality Service Award and COVID-19 Resilience Medal, he now practises at Spectrum Vascular & General Surgery, offering patient-centred care with a focus on minimally invasive treatment.
A diabetic foot ulcer is an open wound or sore that develops on the foot of someone with diabetes. It often appears on the sole, heel or tips of the toes.
Diabetes can damage the nerves over time. This is called peripheral neuropathy. When this happens, the feet may lose the ability to feel pain, heat or pressure. A blister from a tight shoe, a small cut or repeated pressure from walking can become a wound before the patient notices it.
Diabetes can also narrow the blood vessels. This reduces the flow of oxygen and nutrients to the foot, which may slow wound healing.
About 25 percent of people with diabetes may develop a foot ulcer during their lifetime. In Singapore, about 5 diabetes-related amputations occur each day. Many cases may be preventable with early assessment, timely treatment and regular foot care.
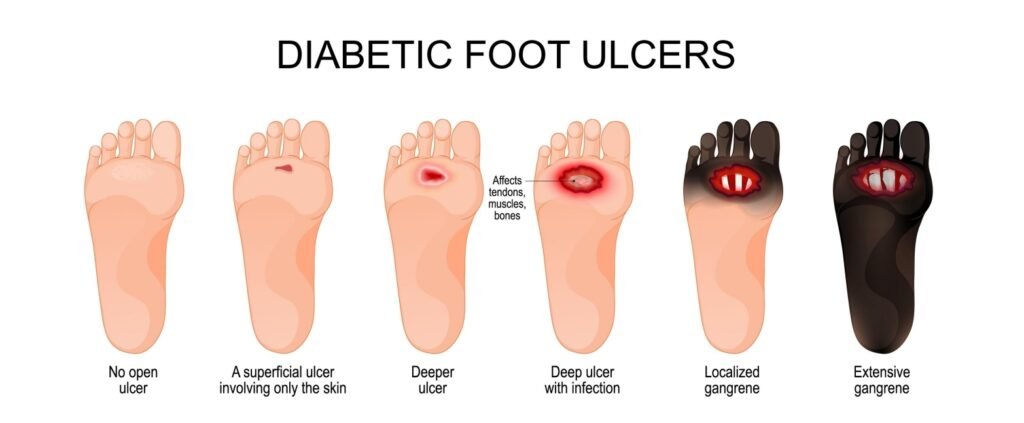
Doctors may use the Wagner grading system to describe the depth and severity of a diabetic foot ulcer. The grade helps guide how urgently treatment is needed.
| WAGNER GRADE | WHAT IT MEANS | ACTION REQUIRED |
|---|---|---|
| Grade 0 | Skin is intact. Early warning signs such as callus or redness may be present. | Arrange a specialist assessment soon. |
| Grade 1 | Shallow ulcer affecting the skin surface. | See a specialist within days. |
| Grade 2 | Deep ulcer reaching tendon, joint capsule or bone. | Seek urgent specialist assessment. |
| Grade 3 | Deep ulcer with abscess or bone infection. | Hospital assessment may be required. |
| Grade 4 | Gangrene affecting the toes or front of the foot. | Seek same-day medical attention. |
| Grade 5 | Gangrene affecting the whole foot. | Seek emergency medical attention. |
Seek medical attention promptly if you have diabetes and notice a foot wound.
Diabetic nerve damage can reduce pain as a warning sign. A painless wound is not always a minor wound. Some ulcers can worsen without causing much discomfort, especially when infection or poor circulation is present.
Diabetic foot ulcers often develop because of a combination of nerve damage, poor blood supply, pressure on the foot and infection.
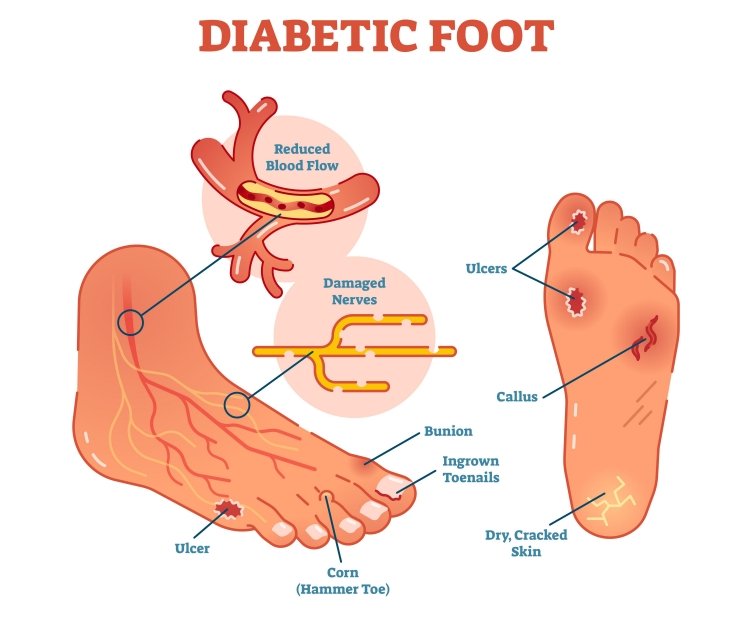
High blood sugar can damage the small nerves in the feet over time. This may reduce the ability to feel pain, heat and pressure. A stone in a shoe, a blister or
friction from a tight sock may then go unnoticed until a wound forms.
Diabetes can cause fatty deposits to build up inside the arteries. This can narrow the arteries and reduce blood flow to the feet.
Poor blood supply is an important factor in wound healing. If the wound does not receive enough blood, oxygen and nutrients, it may take longer to heal or may not improve with dressings alone.
Learn more about peripheral arterial disease on our arterial disease page.
Repeated pressure on the sole, toes or heel can cause the skin to break down. Foot deformities such as claw toes, bunions or Charcot foot may create pressure points. Callus can build up over these areas and later crack open into an ulcer.
Once the skin is broken, bacteria can enter the wound. People with diabetes may have a slower immune response, which can allow infection to spread. Infection may involve the surrounding tissue or, in more serious cases, the bone. Bone infection is called osteomyelitis and usually requires more complex treatment. Learn more about chronic wound care at our clinic.
Adequate blood flow plays an important role in wound healing. Blood carries oxygen, immune cells and nutrients that help repair damaged tissue and fight
infection.
When peripheral arterial disease narrows or blocks the arteries, less blood reaches the foot. The wound may appear clean on the surface but still fail to close because the underlying circulation is poor.
Some patients receive wound dressings for weeks or months without improvement because the blood supply has not yet been assessed. A vascular assessment helps determine whether circulation is contributing to delayed healing.
Dr Tay assesses and treats underlying arterial disease where present. Where appropriate, treatment to improve blood flow may support wound healing and
reduce the risk of further complications.
Critical Limb-Threatening Ischaemia (CLTI) occurs when blood flow to the foot is severely reduced and the limb is at risk.
Patients with CLTI may have rest pain, non-healing ulcers or gangrene. It requires urgent vascular assessment because the risk of major complications, including amputation, can be higher without timely treatment.
During the first consultation, the blood supply to the foot is assessed before a treatment plan is recommended.

Ankle Brachial Index, or ABI, is a simple bedside test that compares blood pressure
at the ankle with blood pressure in the arm. A low reading may suggest narrowed
arteries and reduced blood flow to the foot.
Duplex ultrasound is an imaging scan that maps blood flow in the arteries. It helps
identify where narrowing or blockage may be present.
An angiogram may be recommended when a procedure to improve blood flow is being considered. It provides a detailed map of the arteries from the hip to the foot and helps guide treatment planning.
If poor circulation is contributing to delayed wound healing, treatment to improve blood flow may be considered.
Angioplasty is a minimally invasive procedure where a small balloon is guided into a narrowed or blocked artery and inflated to improve blood flow.
A stent may sometimes be placed to help keep the artery open. It is often performed under local anaesthetic and some patients may go home on the same day.
Bypass surgery may be considered when the blockage is not suitable for angioplasty. A new route for blood flow is created around the blocked artery, often using a vein from the patient’s own leg.
After circulation is improved, wound healing may progress more effectively when combined with wound care, infection control and pressure relief.

Accurate diagnosis means assessing both the wound and the blood supply behind it. At Spectrum Vascular and General Surgery, the assessment looks at the ulcer, circulation, sensation and signs of infection.
Some patients present after prolonged wound care without a vascular assessment. Checking blood flow is an important part of understanding why the wound is not healing.
Treatment for a diabetic foot ulcer usually involves several parts. These may include wound care, infection control, pressure relief and treatment to improve blood flow where needed.
Debridement removes dead, infected or hardened tissue from the wound. This helps create a cleaner wound base and may support healing.
Dr Tay may perform sharp debridement in clinic or in theatre, depending on the wound. For many patients with nerve damage, the procedure may cause little or no pain.
Do not apply antiseptic creams, betadine or hydrogen peroxide to an open diabetic ulcer unless advised by your doctor. These products may irritate fragile healing tissue. Specialist-directed wound care is recommended.
Offloading means reducing pressure on the wound. This is important because repeated pressure from walking can delay healing.
Offloading options may include:
The right option depends on the wound location, foot shape, infection status and the patient’s overall condition.
If infection is suspected, a wound swab may be taken to identify the bacteria present. Antibiotics can then be selected based on the results.
For bone infection, treatment may include intravenous antibiotics, oral antibiotics
and, in some cases, surgery to remove infected or dead tissue. The treatment plan
depends on the severity and extent of infection.
When poor blood supply is contributing to a non-healing wound, improving
circulation may be an important part of treatment.
Revascularisation refers to procedures that restore or improve blood flow. These
may include angioplasty or bypass surgery. Dr Tay performs these procedures
where indicated as part of a treatment plan for patients whose ulcers are linked to
narrowed or blocked arteries.
Wound dressings alone may not be enough when circulation is poor. A vascular
assessment helps determine whether revascularisation may be appropriate.
Once blood flow and infection are addressed, advanced wound care may be
considered to support closure.
Options may include:
The choice depends on the wound condition, blood supply, infection status and overall health of the patient
If gangrene affects the toes or part of the foot, surgery may be needed to remove
non-viable tissue. In selected cases, limited removal of affected tissue may help preserve more of the foot and support walking function.
The treatment plan is based on circulation, infection control and the amount of
tissue affected.
Many diabetic foot ulcers may be managed without major amputation when they are assessed and treated early.
Amputation may be considered when blood flow cannot be improved, infection cannot be controlled or tissue damage is too extensive. In many patients, treatment focuses on controlling infection, improving blood flow where possible and preserving function.
Even some advanced ulcers with limited gangrene may be managed with a limb preservation approach when circulation can be improved and infection is controlled. A vascular assessment helps determine the available treatment options.
Healing time depends on the depth of the wound, blood supply, infection, pressure on the wound and the patient’s overall health.
A superficial ulcer with good blood flow may heal within 6 to 12 weeks with appropriate care. Deeper ulcers, infected wounds or ulcers with poor circulation
may take significantly longer.
Blood supply is an important factor in healing. A wound with adequate circulation has a better chance of improving with wound care. A wound with poor circulation may heal slowly or fail to improve until blood flow is assessed and treated where appropriate.
| WOUND STAGE | TYPICAL HEALING TIMELINE |
|---|---|
| Grade 1 ulcer with good blood flow | Around 6 to 12 weeks with appropriate care |
| Grade 2 to 3 ulcer with infection | May take 3 to 6 months or longer |
| Grade 3 to 4 ulcer with bone infection or gangrene | Urgent assessment is needed. Healing depends on infection control, circulation and treatment response. |
Blood sugar control
High blood sugar can slow the body’s ability to repair tissue. For many patients, keeping HbA1c below 7 percent may support wound healing, although targets
should be personalised by the treating doctor.
Smoking
Smoking narrows blood vessels and reduces oxygen delivery to the wound. Stopping smoking may improve circulation and support healing.
Offloading compliance
Continuing to walk on the wound can delay healing. Following offloading advice is an important part of treatment.
Diabetic foot ulcers can return after they heal. Prevention requires ongoing foot care, pressure control and diabetes management.
For everyday habits that protect your feet, see our guide on caring for your diabetic foot at home.
Not all foot and leg ulcers are the same. The right treatment depends on the cause. An accurate diagnosis is important before starting treatment.
| FEATURE | DIABETIC FOOT ULCER | VENOUS LEG ULCER | ARTERIAL ULCER |
|---|---|---|---|
| Where it forms | Sole, toes or heel, often over pressure points | Lower leg, often around the ankle | Toes, between toes or heel |
| Pain level | May be painless because of nerve damage | Aching or heavy sensation | Often painful, especially when circulation is poor |
| Wound appearance | Deep, punched out or with callused edges | Shallow with irregular edges | Deep with a pale base or clean edges |
| Surrounding skin | Dry or callused | Swollen with brown staining | Thin, shiny, cool or hairless |
| Main cause | Nerve damage and poor circulation | Venous insufficiency | Peripheral arterial disease or CLTI |
| Key diagnostic test | ABI and monofilament test | Duplex venous ultrasound | ABI and arterial imaging |
| Primary treatment | Debridement, offloading, infection control and revascularisation where needed | Compression therapy and wound care | Vascular assessment and revascularisation where appropriate |
Some patients with diabetes may also have varicose veins or peripheral artery disease. A proper assessment can help identify the cause of the ulcer and guide treatment.
Some small wounds may improve, but it is not safe to wait and see. Most diabetic foot ulcers need medical assessment, wound care, pressure relief and blood supply evaluation. Early care may reduce the risk of infection and other complications.
No. Soaking may soften fragile wound tissue and introduce bacteria. A diabetic foot ulcer should be cleaned and dressed according to medical advice. Do not soak the wound unless your doctor specifically tells you to.
A superficial ulcer with good blood flow may heal in 6 to 12 weeks with appropriate care. Deeper ulcers, infected wounds or ulcers with poor circulation may take longer. A vascular assessment can help identify whether reduced blood flow is delaying healing.
Yes. Diabetes can damage the nerves in your feet, which means a wound may not hurt even if it is serious. If you notice an open sore on a diabetic foot, arrange medical assessment promptly.
Both may be involved in care. A podiatrist helps manage the wound surface, pressure relief and footwear. A vascular surgeon assesses blood flow and treats narrowed or blocked arteries where needed. If an ulcer is not improving, a vascular assessment is important.
Bone infection is called osteomyelitis. It is diagnosed with MRI or bone biopsy and treated with a prolonged course of targeted antibiotics, typically 6 weeks or longer. When caught early, osteomyelitis does not automatically lead to major amputation.
Not every diabetic foot ulcer leads to amputation. Many ulcers can be managed with wound care, infection control, pressure relief and vascular treatment where appropriate. The risk depends on blood flow, infection, tissue damage and how early treatment begins.
A normal wound usually causes pain and has enough blood supply to support healing. A diabetic foot ulcer may not hurt because of nerve damage. It may also heal slowly if blood flow is reduced. This is why standard wound care alone may not be enough for some diabetic foot ulcers.
If you or someone you care for has diabetes and a foot wound that is not healing, arrange an assessment. This is especially important if the wound is worsening, has discharge, smells unpleasant or is linked to redness, swelling, fever or black tissue.
Early vascular assessment may help identify circulation problems and guide timely treatment.
Dr Tay Jia Sheng and the team at our vascular clinic in Singapore provide assessment and treatment for diabetic foot ulcers and related vascular conditions.
For enquiries, consultation or second opinions, please complete the form below or call us at +65 8874 0371.
Our team will get back to you shortly to assist with your request.

38 Irrawaddy Road
#10-33
Singapore 329563
Tel: +65 6041 0933
1 Farrer Park Station Road
#08-14 Connexion
Singapore 217562
Tel: +65 6974 8859
HP: +65 8874 0371 (24 hours)
Email: co*****@**************ry.com
© 2026 Spectrum Vascular & General Surgery